
07 Jun Lumbar Spine Surgery is Becoming an Overnight Surgical Procedure for Most Patients
Lumbar Spine Fusion was developed decades ago as a method to stabilize the lumbar spine after tumor resection, traumatic injuries, degenerative disease, and scoliosis. Over the past 10 years, lumbar spinal fusion surgery (1-level & 2-level) has become an overnight procedure. Patients are now discharged the next day after surgery. Those patients with a long history of pain medication usage, chronic pain symptoms, or significant risk factors for complications may stay in the hospital longer.
Criteria that matter for early discharge include age, history of narcotics for pain, functional level prior to surgery, cardiac history, pre-operative symptoms such as weakness or excessive pain. Here are some of the reasons why lumbar fusion is heading towards an ambulatory procedure when you have surgery through the Lumbar Spine Center.
Positioning with the Jackson Table
Patients are positioned with the Jackson Table that allows the abdomen to fall away from the spine while prone (face down) reducing the pressure on the spinal venous plexus thereby reducing the amount of blood loss during surgery.

Cell Saver
Although we do not expect much blood loss, we use two cell saver suctions. The blood suctioned and lost during surgery is aspirated into canisters by the Cell Saver Machine and filtered to give back to the patients after surgery. In approximately 50% of the surgical procedures, we give the patients 100 ml – 150 ml of their own blood. It is our feeling that the blood helps with mobility after surgery and allows them to go home sooner.

Intraoperative CT Scan with Navigation
After the patient is asleep, we make the incision in the lower back and expose the posterior lumbar spine. Once exposed, we attach a Navigation Localizer and then bring in the CT Scanner or O-Arm to obtain an intraoperative CT Scan. After we perform a CT Scan, the images are sent to a Computer Workstation. The Workstation integrates the CT Scan Images to register with the space of the patient using the Navigation Localizer. When we use the pointer from the Workstation, it shows us exactly where we are pointing relative to the CT Scan images making pedicle screw placement much easier, more accurate and safer. The CT Scan is repeated after the placement of the pedicle screws and before the incision is closed to make sure they are in properly.

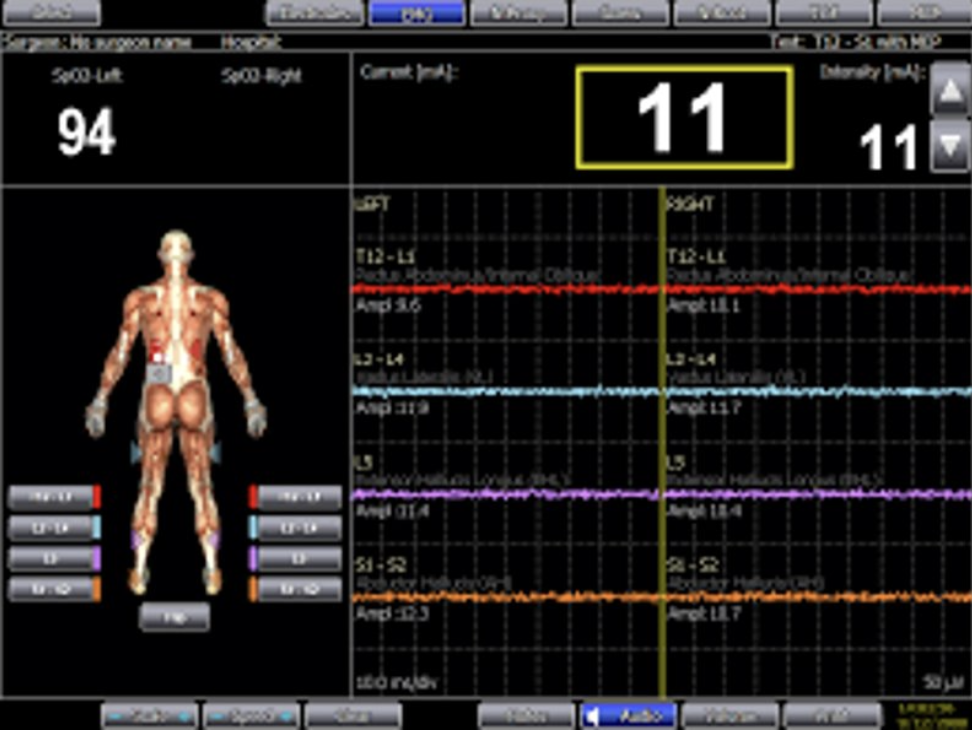
Intraoperative Monitoring
Once the patient is asleep, a Neuromonitoring Technician places electrodes into the muscle of the legs and arms to measure the signal conduction of the brain to the limbs during the surgical procedure. The technician monitors the impulses throughout the procedure reporting to an interpreting Physician from a remote location. During the surgery, if there is undue pressure on a nerve, the technician will alert the surgeons. Additionally, while we insert the pedicle screws, we are monitoring the screw as it is going into the pedicle bone to make sure it is not inadvertently placed too close to a nerve.
Power Tools
The majority of the pedicle screws placed are from Medtronic Spine. Medtronic provides a power drill (Powerease) that makes placing screws easier.

Bone Grafting Techniques
During your surgery, we collect bone graft (autograft) in removing the lumbar lamina through handheld instruments and bone shavings from using a high-speed drill. In particular, Dr. Abrahams uses the BDC-15, an FDA approved device that he developed to increase the volume of the patient’s bone thereby reducing the need for any cadaver bone (allograft). We use the BDC-15 Device with in-line suction.

Collected Bone Graft
During this surgical procedure, we collected 20 ml of autograft from the patient.








